By Ana B. Ibarra, CalMatters
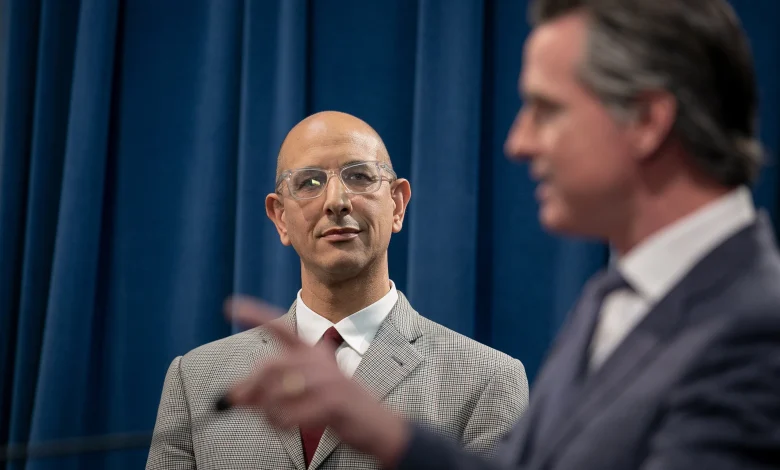
California Health and Human Services Agency Secretary Dr. Mark Ghaly looks on as Gov. Gavin Newsom gives a press conference at the state Capitol in Sacramento, following the first COVID-19 death in the state, on March 4, 2020. Photo by Anne Wernikoff for CalMatters
This story was originally published by CalMatters. Sign up for their newsletters.
As states figure out how to adjust to federal funding cuts, policy shifts, and major Medicaid shakeups, 2026 will be pivotal for California health officials and lawmakers.
Many Californians on Medicaid, better known here as Medi-Cal, already struggle to access timely and quality care. Now, experts warn that millions more could lose coverage under H.R.1, which makes sweeping changes to the country’s safety net programs.
Anticipating the fallout, a group of health foundations has formed the Future of Medi-Cal Commission. Its charge: creating a 10-year blueprint for a program that covers more than 14 million low-income residents and pays for key services from childbirth to nursing home care.
The commission’s co-chairs are Gov. Gavin Newsom’s former chief of staff Ann O’Leary and his former Health and Human Services Secretary Dr. Mark Ghaly, who led the state’s response to the COVID-19 pandemic.
The 29-member commission will begin meetings in January and will deliver recommendations in early 2027.
Ghaly spoke to CalMatters about the commission and the challenges ahead. “Nothing forces you to think about these things more than the threat to your current existence,” Ghaly said.
This conversation has been edited for length and clarity.
What’s the origin story for this commission? Who decided it needs to exist and why?
The health foundations collectively that focus on programs like Medicaid and think about issues of equity … came together and said, “we’ve got to react and be prepared for the immediate shifts.” This is a forcing function moment – and a state like California for its millions of people who benefit from Medi-Cal but also the nation have got to drive some process to consider: what does this all mean for the mission of supporting low-income people to be healthy and well?
Obviously H.R. 1 makes a lot of changes. What do you see as the biggest challenge for Medi-Cal right now?
There’s this big concern that a lot of people who have become confident and comfortable in their care may lose it, either through eligibility or if there are – God forbid – service cuts. Those are the things that I think are the “now” worries. The future worries are a little bit different. They include some of the things I just mentioned, but it’s also about sustainability and the growth and the cost of the program, and how we are sure we’re doing the right things that actually drive health outcomes to be better.
Speaking of costs, the Medi-Cal program has grown extensively over the last several years — some people say it’s grown too much, and earlier this year, the program went over budget. At which point does the program become too big?
Look, Medi-Cal has become a true health program, not just a health care program. [What that means is,] it’s really thinking about all the things that go into creating healthy individuals, healthy families, healthy communities, and, by extension, a healthier state.
Has it grown too big? I think the piece of that that I appreciate and think is very important to dig into, is, are we doing all the things that matter? It’s great that we’re doing things to support health broadly, but are all the things that we’re paying for and creating the workforce for the things that make sense to do? I think that’s what is going to be a very interesting piece [for] this commission to dig into.
The state is freezing enrollment and cutting benefits already because of budget pressures. Are more service cuts and kicking people off the program in order to respond to the federal shifts inevitable?
It’s a hard question to respond to without the knowledge of what the other pressures are that the state’s going to face. You never want to say never, but I know this governor, I know the team there. They’re not going to want to make those kinds of cuts and decisions. But at the end of the day, the state has a responsibility with its budget to make sure it’s well and balanced.
What do you expect to happen to the commission’s recommendations?
I would like to think that what the commission writes and ends up with is something that is usable by policymakers.
What I like about the commission’s makeup, in part, is that it is a lot of operators. It’s a lot of people who can understand how the high level idea might actually get implemented on the ground and through the different channels and levels of bureaucracy, which is a very big plus.
By the time the commission delivers its report, California will have a new governor. What should the next governor be thinking about and saying about these problems?
I would love our candidates to be really hungry to understand what they might come in and expect to do to support improving, modernizing and ensuring that California’s flagship Medi-Cal program is maintained and supported.
If you find a somewhat sophisticated candidate, and then elected governor, in the healthcare space, they’re going to see how it’s not that all roads lead to Medi-Cal, but Medi-Cal is a major freeway in the healthcare environment, and it is the one that she or he has the choice to really influence and control.
I’ll just add one other thing. Health care is a huge piece of the California economy. And I don’t mean just Medicaid; I mean broadly. Most every person in California thinks about, “How do I secure and preserve access to health care and live in a healthy community?” I think those are important priorities.
This article was originally published on CalMatters and was republished under the Creative Commons Attribution-NonCommercial-NoDerivatives license.